


ADVERTISEMENT
Percutaneous Valve Innovations: Transcatheter Mitral Valve Intervention
Can you tell us about your center and history with the mitral valve?
 NorthShore’s valve program goes back to the beginning use of MitraClip (Abbott Vascular) in 2003. We did the first MitraClip procedure in the United States, and I have been the principal investigator for the EVEREST (Endovascular Valve Edge-to-Edge REpair Study) MitraClip trials. Prior to the MitraClip, I was involved with the Inoue balloon (Toray Medical) mitral valvuloplasty trial, going back to 1990, which became the only device approved for mitral valvuloplasty. It remains the standard therapy for mitral stenosis worldwide.
NorthShore’s valve program goes back to the beginning use of MitraClip (Abbott Vascular) in 2003. We did the first MitraClip procedure in the United States, and I have been the principal investigator for the EVEREST (Endovascular Valve Edge-to-Edge REpair Study) MitraClip trials. Prior to the MitraClip, I was involved with the Inoue balloon (Toray Medical) mitral valvuloplasty trial, going back to 1990, which became the only device approved for mitral valvuloplasty. It remains the standard therapy for mitral stenosis worldwide.
What studies are you currently involved in?
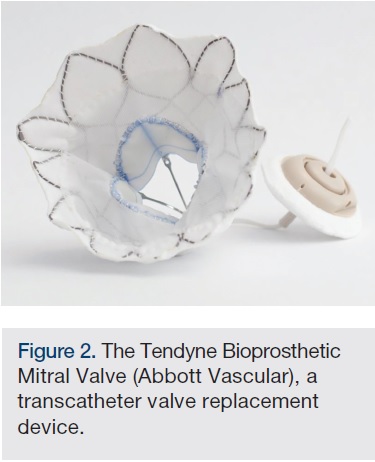
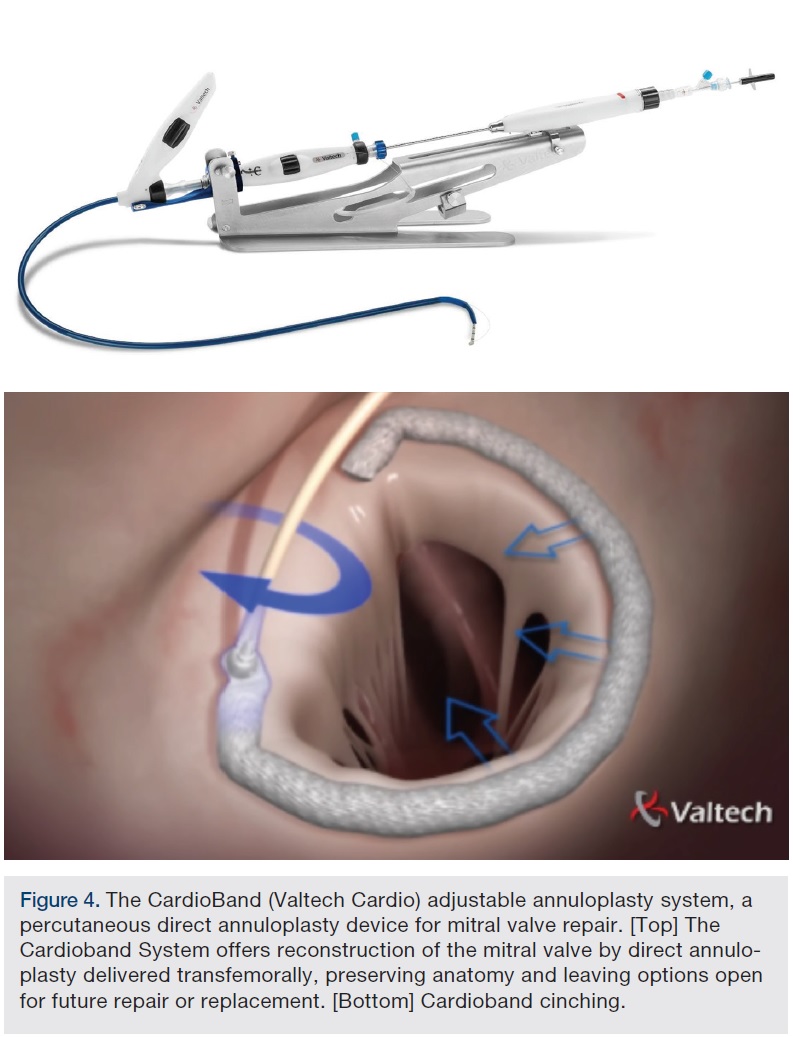
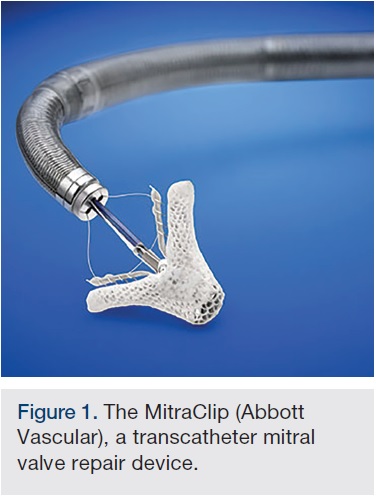 We have an investigator-sponsored investigational device exemption (IDE) study for using the Edwards transcatheter aortic valve replacement (TAVR) device in calcific mitral stenosis, MITRAL (Mitral Implantation of TRAnscatheter vaLves), headed nationally by my colleague Mayra Guerrero. We are also participating in the Tendyne (Abbott Vascular) mitral valve replacement trial. I am anticipating several trials for other mitral repair devices that are in use internationally, including the Carillon Mitral Contour System (Cardiac Dimensions) and the CardioBand System (Valtech Cardio). Ongoing is the COAPT trial (Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy for Extremely High-Surgical-Risk Patients). The trial was originally intended to randomize 430 patients, but an interim analysis several months ago showed that the event rate was not high enough to reach a conclusion, so the enrollment has been extended. It will be another several months for COAPT to finish enrollment.
We have an investigator-sponsored investigational device exemption (IDE) study for using the Edwards transcatheter aortic valve replacement (TAVR) device in calcific mitral stenosis, MITRAL (Mitral Implantation of TRAnscatheter vaLves), headed nationally by my colleague Mayra Guerrero. We are also participating in the Tendyne (Abbott Vascular) mitral valve replacement trial. I am anticipating several trials for other mitral repair devices that are in use internationally, including the Carillon Mitral Contour System (Cardiac Dimensions) and the CardioBand System (Valtech Cardio). Ongoing is the COAPT trial (Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy for Extremely High-Surgical-Risk Patients). The trial was originally intended to randomize 430 patients, but an interim analysis several months ago showed that the event rate was not high enough to reach a conclusion, so the enrollment has been extended. It will be another several months for COAPT to finish enrollment.
Are there advantages to mitral valve replacement vs repair? Will one or the other dominate in the future?
The appeal of mitral replacement is the promise of complete elimination of any residual mitral regurgitation (MR), while the appeal of the repair technologies is established safety and relative simplicity. How this balance unfolds will take at least several years.
Are trials looking at both functional and degenerative MR?
 All of the new device trials are targeting mainly high-risk patients with functional MR. COAPT is looking at functional MR. Tendyne is mixed, so it is including both functional and degenerative MR, and the population is defined as largely being unsuitable for other therapies. The MITRAL trial is for calcific mitral stenosis; that group usually has mixed mitral stenosis/MR, and it is a very distinct group compared to the typical heart failure/functional MR population, which is the largest population for the MR device trials.
All of the new device trials are targeting mainly high-risk patients with functional MR. COAPT is looking at functional MR. Tendyne is mixed, so it is including both functional and degenerative MR, and the population is defined as largely being unsuitable for other therapies. The MITRAL trial is for calcific mitral stenosis; that group usually has mixed mitral stenosis/MR, and it is a very distinct group compared to the typical heart failure/functional MR population, which is the largest population for the MR device trials.
How does the anatomy of the mitral valve impact device design?
The mitral valve orifice is much bigger than the aortic valve orifice. It is D-shaped, so creating a replacement prosthesis for the mitral valve requires a much bigger device and a much more complex geometry. That is one of the challenges of mitral valve replacement efforts. The calcific mitral stenosis population tends to have a much smaller orifice, because of the presence of calcification, which, in highly selected cases, makes it possible to put in an aortic valve prosthesis.
What are some of the challenges of transcatheter therapy in the mitral valve?
 On the positive side, catheter therapy has been successfully applied in patients who are at prohibitive risk for surgery. That plus has already been realized. The larger challenges are that the dedicated mitral devices are currently larger profile. Almost all of the successful procedures have been done transapically. For the long haul, we can all expect that these procedures will have to be transseptal to truly reach their full promise in terms of treating larger numbers of patients. It is not just a matter of decreasing the bulk the devices. Transseptal delivery is harder in terms of geometric alignment of the devices, in terms of achieving a stable position and the correct axis for the device to sit properly. From the apex, you have a short, straight shot, and getting the devices to align is much more achievable from a technical standpoint, but, of course, it is harder on the patient to have an apical rather than a transseptal procedure. One of the biggest challenges, where the magnitude of the challenge has been bigger than anticipated, is the potential for the mitral devices to protrude into the left ventricular outflow tract and obstruct aortic outflow. Device protrusion into the left ventricular outflow tract and obstruction of aortic outflow has turned into an important limitation of many mitral replacement devices. The fact that this has been recognized has forced the rapid development of CT scan model planning for these procedures. CT scanning, as with TAVR, has become integral to the planning of mitral procedures.
On the positive side, catheter therapy has been successfully applied in patients who are at prohibitive risk for surgery. That plus has already been realized. The larger challenges are that the dedicated mitral devices are currently larger profile. Almost all of the successful procedures have been done transapically. For the long haul, we can all expect that these procedures will have to be transseptal to truly reach their full promise in terms of treating larger numbers of patients. It is not just a matter of decreasing the bulk the devices. Transseptal delivery is harder in terms of geometric alignment of the devices, in terms of achieving a stable position and the correct axis for the device to sit properly. From the apex, you have a short, straight shot, and getting the devices to align is much more achievable from a technical standpoint, but, of course, it is harder on the patient to have an apical rather than a transseptal procedure. One of the biggest challenges, where the magnitude of the challenge has been bigger than anticipated, is the potential for the mitral devices to protrude into the left ventricular outflow tract and obstruct aortic outflow. Device protrusion into the left ventricular outflow tract and obstruction of aortic outflow has turned into an important limitation of many mitral replacement devices. The fact that this has been recognized has forced the rapid development of CT scan model planning for these procedures. CT scanning, as with TAVR, has become integral to the planning of mitral procedures.
Why does the device protrusion occur?
The mitral inflow and the left ventricular outflow are normally adjacent, and there are two ways that the left ventricular outflow can be compromised by a mitral device. One is directly. The mitral devices have to protrude to some degree into the ventricle in order to anchor, and the more they protrude, the more likely they are to push into the left ventricular outflow tract. The second mechanism is that the native anterior mitral leaflet can be displaced into the left ventricular outflow tract. Thrombus formation on the devices is another problem, and in fact, it has been an issue since the first commercial mitral valve surgical replacement device was developed in the 1960s. The left atrium is a much lower flow chamber than the left ventricle and aorta, and the mitral devices have more prosthetic material, and thus thrombus formation on these devices is an important problem. In the mitral space, for example, the Edwards Fortis program was discontinued in part because of thrombus formation on the devices, which occurred despite anticoagulation therapy. The need for anticoagulation is another important challenge for treating patients with these mitral devices.
What are the next steps for developing mitral replacement devices?
 In terms of development, all or most of the companies that are involved in this effort are working to develop effective transseptal delivery systems. It is a challenge to make a large-caliber device predictably deliverable from the left atrial side, rather than the left ventricular side.
In terms of development, all or most of the companies that are involved in this effort are working to develop effective transseptal delivery systems. It is a challenge to make a large-caliber device predictably deliverable from the left atrial side, rather than the left ventricular side.
How will imaging continue to develop?
Patient selection and procedure planning are driven by computed tomography (CT). The use of CT for assessing mitral geometry and virtual valve implantation has rapidly become the standard approach. Software analysis packages to make these assessments, which have become the standard for TAVR CT analysis, are under development. Most mitral procedures are done with transesophageal echo (TEE) and fluoro interprocedurally, and for many procedures, the essential steps of anchoring the valve and orienting the valve at the key part of the procedure are predominantly echocardiographic. There are some commercial systems available that allow the echo and fluoroscopy images to be fused, and they are going to be helpful, but aren’t yet uniformly available. Imaging has really moved the whole structural heart field at every step, so we will see more and more development of hybrid imaging. There are systems that allow previously acquired CT images to be fused with fluoro images, and these are all very helpful. Historically, the most rudimentary form of imaging has been roadmapping with fluoroscopy, where a static reference can be displayed on a screen and a live image watched in an overlay. Multimodality imaging, having two completely different imaging modalities for guidance, is very exciting in that regard.
How do you see the heart team organizing around the mitral patient?
The heart team has developed, but in an evolutionary manner. You don’t just put together a roster of interested parties, instantly sit down in a room, and have a functioning heart team. In our program, the heart team started many years ago with patient selection for the SYNTAX and EVEREST trials. We now have a Wednesday afternoon weekly heart team meeting, where we review with our research and clinical nursing team, and our interventional and surgical physicians, a list of aortic, mitral, and left atrial appendage patients that are all undergoing screening and procedure planning. In many respects, that is the easiest part. There is an ongoing interaction among the team members at many stages. It becomes part of the whole practice. Our interaction with the surgeons has evolved and in terms of decision-making, it’s not only that it is team-oriented, but that it is a process. Decisions are not usually made in one step, because the evaluation takes face-to-face visits with both the interventional and surgical physicians, and the imaging has to be reviewed. So we need to do whatever it takes to get those major components all to drive toward a decision about best therapy for an individual patient.
What evolution do you see for the team during the procedure itself?
For TAVR, the surgeon and interventional physicians are required to be physically present for Medicare reimbursement. From one program to another, the degree to which both specialties are truly involved in the procedure varies. In our own practice, we have made a serious effort as the procedure has become less surgical to get our surgeon colleagues involved in some of the interventional steps, so that everybody can truly participate in the procedures. On the mitral replacement side, the procedures now are predominantly apical, so there is an obvious clear involvement of the surgeon. This is a work in evolution, so we will see how this changes as the mitral procedures become more percutaneous and less surgical. That is going to be a long road.
Can you talk about the role of the echocardiographer and their interaction with the interventionalist?
For the interventionalist to perform the procedure, an additional imaging specialist is required for echocardiography. For MitraClip, in many institutions, the cardiovascular anesthesiologist is managing the TEE, but it is very institution-specific. In our own program, it is a cardiologist echocardiographer who does the TEE. The learning curve for both the echo and interventional physician is critical, because each has to learn a great deal of new information to be able to take advantage of the echo during an intervention. Historically, there is no single language that both the echo and fluoro imaging interventional physicians have used, so communication and the ability to manage the interaction are key. The interventionalist absolutely has to be able to understand the echo imaging in real time. The demand for the interventional physician to learn CT interpretation has also been a big part of becoming involved with these therapies.
Can you share more about the applications of CT in the planning phase?
Three-dimensional (3D) modeling and rendering by CT that shows the appearance and placement of virtual valves is now part of the evaluation. It has become a common part of the mitral procedure planning for mitral replacement devices. On the aortic side, commercial software has developed to the point where there are several companies with TAVR software packages that will show you a virtual valve. Some programs have an option for importing an STL file, which is a CAD file that describes the specifics of a particular device, so it’s not just that you put a generic cylinder into the valve orifice in the 3D rendering, but rather a specific type of aortic or mitral valve. On the mitral side, this is not as well developed. It is critical to recognize how early the mitral valve replacement effort is. We have hundreds of thousands of TAVR implants, so that the experience, resources, and impetus to develop software and analytic programs are huge on the aortic side. On the mitral side, the total number of patients treated with replacement devices, the dedicated mitral devices, is still barely 100 patients worldwide. Most of the software is homemade, and there are companies working on mitral software packages, but those are programs that are in development.
Any final thoughts?
Patients who either had no option or were facing an open sternotomy procedure are now being treated with increasing frequency with a completely percutaneous procedure, a short hospital stay, and a remarkably short recovery time. It is exciting to do these procedures to replace or repair a valve, and now, for TAVR, to do so in an awake patient. For mitral, we are at the beginning of that journey, but with a lot of that same promise, typically validated on the one-month follow-up visit where these patients come for follow-up and they are transformed, without having had open surgery.
Disclosure: Dr. Feldman reports research grants and honoraria from Abbott, Boston Scientific, Edwards Lifesciences, and W.L. Gore.
Dr. Ted Feldman can be contacted at tfeldman@tfeldman.org.
