


ADVERTISEMENT
Entrapment and Retention of a Ruptured Coronary Angioplasty Balloon
1Department of Internal Medicine, Danbury Hospital, Western Connecticut Health Network, Danbury, Connecticut; 2Section of Cardiovascular Medicine, Yale-New Haven Hospital, Yale University School of Medicine, New Haven, Connecticut
This article received a double-blind review from members of the Cath Lab Digest Editorial Board.
Disclosures: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Dr. Robby Wu at rzw113@gmail.com.
•Note: A correction to this article has been made from the print version.
Abstract
The entrapment of angioplasty device fragments is an increasingly rare consequence of percutaneous coronary intervention. Whenever possible, percutaneous retrieval should be favored as the treatment of choice. In certain clinical scenarios, however, retention of the foreign object within the coronary vessel may be the most appropriate option. Here we report a case of a ruptured angioplasty balloon that was entrapped in the posterior descending artery of the right coronary artery and retained in situ after multiple failed attempts at percutaneous retrieval. The patient was placed on aspirin and warfarin, and at 3-month follow-up, has not suffered any adverse consequences related to her retained balloon.
Introduction
Device entrapment is a rare consequence of modern-day percutaneous coronary intervention (PCI), with a reported incidence of less than 1%.1 Growing knowledge of interventional techniques and advances in retrieval devices have helped to decrease the 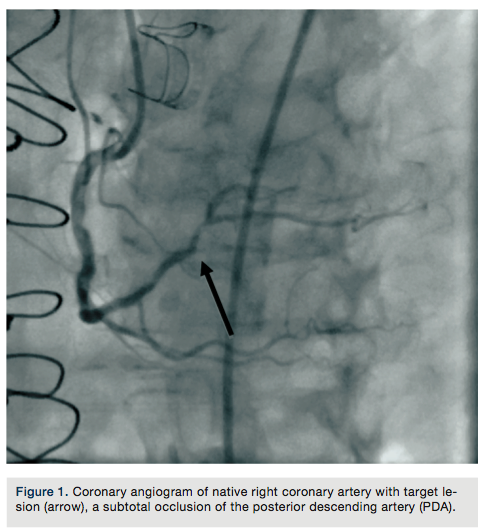 need for emergency surgical therapy, but management of the hemodynamically stable patient often remains in question. Due to the scarcity of this complication, available literature is quite limited. Here we present a case where a ruptured angioplasty balloon was entrapped in the right coronary artery and was retained in situ.
need for emergency surgical therapy, but management of the hemodynamically stable patient often remains in question. Due to the scarcity of this complication, available literature is quite limited. Here we present a case where a ruptured angioplasty balloon was entrapped in the right coronary artery and was retained in situ.
Case report
A 75-year-old female with a past medical history of coronary artery disease with previous coronary artery bypass grafting with left internal mammary artery (LIMA) to left anterior descending (LAD) artery, saphenous venous graft (SVG) to ostial medial (OM) branch, SVG to postero-lateral (PL) branch, and bioprosthetic aortic valve replacement presented with progressive dyspnea on exertion associated with substernal chest pressure. She presented with no ECG changes or elevation in cardiac biomarkers. Despite optimal medical management, she continued to endorse chest pain and thus underwent cardiac catheterization for evaluation of her coronary anatomy. Catheterization revealed a patent LIMA to LAD and SVG to OM, moderate disease in the SVG to PL graft, and a new, severe subtotal occlusion of the posterior descending artery (PDA) from the right coronary artery. We proceeded with intervention to this vessel using a 6 French (Fr) 0.75 Amplatz guide catheter. The index lesion was crossed with a Balance Middle Weight (BMW) guide wire (Abbott Vascular), with difficulty. Predilation was attempted with a 2.5 x 12 mm Apex balloon (Boston Scientific), but could not be advanced beyond the mid PDA. A GuideLiner catheter (Vascular Solutions) and a 1.25 x 10mm Sprinter Legend balloon (Medtronic) were advanced to the distal right coronary artery where they became resistant to advancement. The balloon was briefly inflated, but would still not advance. It was noted to have ruptured and despite aggressive tugging and pushing, could not be removed. The GuideLiner catheter could not be advanced further into the vessel to help free the balloon. It could also not be removed entirely, as it contained the shaft of the balloon. Eventually, with applied tension, the balloon shaft avulsed and remained in the distal RCA. Two different snares and two QuickCross catheters (Spectranetics) were advanced over the guide wire, but could not reach the site of the balloon. Given the tortuous anatomy and degree of calcification, it was determined that no other device or stent could be delivered, and thus the delivery wire was removed. Final angiography revealed TIMI-3 antegrade flow into the PDA, but with an obvious retained balloon tip and associated filling defect. Severe residual stenosis of the index lesion also remained. The patient remained hemodynamically stable throughout the procedure and asymptomatic subsequently. No ECG changes were identified and no regional wall motion abnormalities were seen on 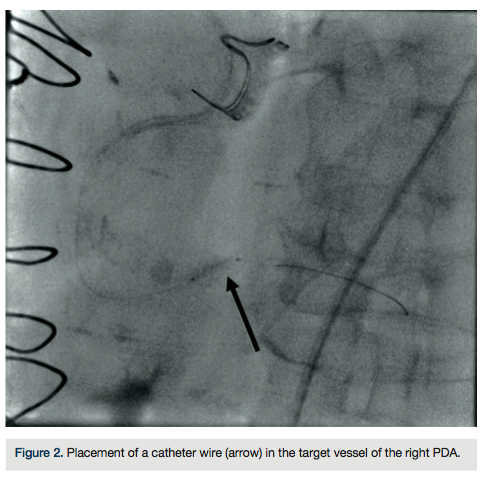 echocardiography. The patient was placed on aspirin and warfarin, and at 3-month follow-up had not suffered any adverse consequences related to her retained balloon. At 3-month follow-up, warfarin was discontinued.
echocardiography. The patient was placed on aspirin and warfarin, and at 3-month follow-up had not suffered any adverse consequences related to her retained balloon. At 3-month follow-up, warfarin was discontinued.
Discussion
Complications during percutaneous coronary intervention (PCI) are rather infrequent, with less than 1% of all cases requiring emergency cardiothoracic intervention.2 Management of entrapped devices during PCI can be frustrating and anxiety provoking. Due to their thrombogenicity, lethal consequences such as myocardial infarction can occur with entrapped devices and thus ischemic, hemodynamically unstable patients often require immediate percutaneous retrieval or even sternotomy and coronary bypass.1 Owing to the scarcity of the complication, however, available literature regarding surgical or medical management for the hemodynamically stable patient is limited. As a result, no formal guidelines exist. While most experts favor removal of any foreign body from the coronary circulation, existing data suggests that catheter remnants or stents do not necessarily mandate removal.3,4 In our case, the patient remained hemodynamically stable with improved flow to the distal PDA and thus, surgical intervention was deferred.
While device entrapment occurs infrequently, balloon entrapment specifically is exceptionally rare, with a recent literature review yielding only eight reported cases over the past two decades.5 Four balloons were retrieved percutaneously and three were removed surgically. While existing literature has documented several cases of retention of fractured guide wires4,12-14, there are very few case reports documenting a ruptured and entrapped angiography balloon being retained in a coronary artery in situ, without any subsequent surgical management.
While many cases are unavoidable, practitioners should be cognizant of hazardous situations that may predispose to balloon entrapment. Heavily calcified (particularly calcified ostial), tortuous, and angulated lesions have been implicated as recurrent 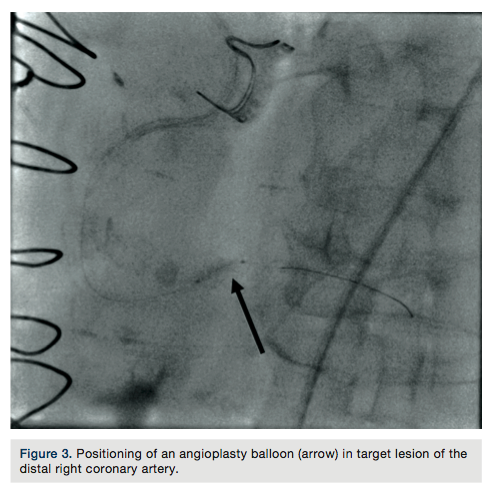 culprits.5,6 Kussmaul et al have further described that fluoroscopic elongation of the balloon can sometimes signify impending balloon failure. Management of the entrapped angiography balloon should be individualized on a case-by-case basis. When possible, percutaneous retrieval should be attempted first.8 Multiple devices are available and despite the infrequency of PCI complications, the interventionalist should become familiar with different retrieval equipment and strategies.9-11 Other than the use of snares, several common techniques can be employed to retrieve entrapped balloons. One technique involves insertion of two or more guide wires into the coronary artery, beyond the area of retained material, before twisting the wires together to produce a helix for retrieval. Another technique involves advancement of a second balloon beyond the retained material, before inflating and pulling back.15 These techniques would not have worked in our case, as the balloon fragment was firmly stuck in a highly calcified and small vessel.
culprits.5,6 Kussmaul et al have further described that fluoroscopic elongation of the balloon can sometimes signify impending balloon failure. Management of the entrapped angiography balloon should be individualized on a case-by-case basis. When possible, percutaneous retrieval should be attempted first.8 Multiple devices are available and despite the infrequency of PCI complications, the interventionalist should become familiar with different retrieval equipment and strategies.9-11 Other than the use of snares, several common techniques can be employed to retrieve entrapped balloons. One technique involves insertion of two or more guide wires into the coronary artery, beyond the area of retained material, before twisting the wires together to produce a helix for retrieval. Another technique involves advancement of a second balloon beyond the retained material, before inflating and pulling back.15 These techniques would not have worked in our case, as the balloon fragment was firmly stuck in a highly calcified and small vessel.
In the event of failed percutaneous retrieval, hemodynamically unstable patients should immediately be transferred for surgical management. Literature suggests that clear recognition of unstable patients and short intervals between failed intervention and emergency surgery leads to improved outcomes.3 One additional option, as demonstrated in our case, is to leave the entrapped device in situ. The few existing case reports of retained guide wire fragments in hemodynamically stable patients have indicated that most do not suffer any adverse sequelae in the long term.4,12-14 Factors that favor retention are if equipment is contained within small, chronically occluded coronary vessels or within a distal segment.4 Subsequent outpatient management has traditionally consisted of either dual antiplatelet therapy, or as in our case, aspirin and an anticoagulation regimen. However, in the absence of conclusive scientific data, any benefits derived from such management are theoretical for now. 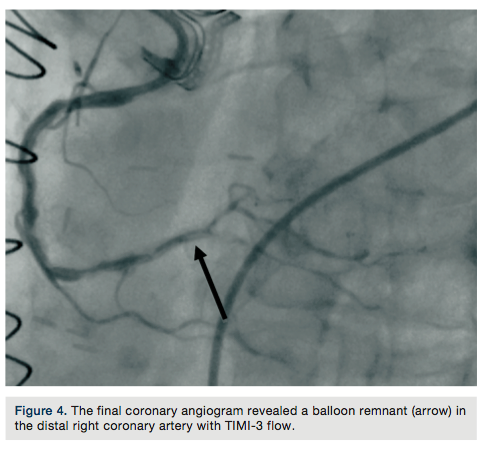
With growing widespread usage of PCI, complications are unfortunately likely to occur. Interventional specialists should be familiar with management strategies for these rare complications.
References
- Iturbe JM, Abdel-karim AR, Papayannis A, et al. Frequency, treatment, and consequences of device loss and entrapment in contemporary percutaneous interventions. J Invasive Cardiol. 2012; 24(5): 215-221.
- Yang EH, Gumina RJ, Lennon RJ, Holmes DR Jr, Rihal CS, Singh M. Emergency coronary artery bypass surgery for percutaneous coronary interventions: changes in the incidence, clinical characteristics, and indications from 1979 to 2003. J Am Coll Cardiol. 2005 Dec 6; 46(11): 2004-2009.
- Alexiou K, Kappert U, Knaut M, Matschke K, Tugtekin S. Entrapped coronary catheter remnants and stents: must they be surgically removed? Tex Heart Inst J. 2006; 33(2): 139-142.
- Hartzler, GO, Rutherford BD, McConahay DR. Retained percutaneous transluminal coronary angioplasty equipment components and their management. Am J Cardiol. 1987; 60(16): 1260-1264.
- Chang WT, Chen JY, Li YH, Tsai LM, Lee CH. A two-case series of entrapment of a ruptured balloon in the coronary artery: Avoidable complications and nonsurgical management. J Formos Med Assoc. 2013 Jun 18. pii: S0929-6646(13)00175-7. doi: 10.1016/j.jfma.2013.05.008.
- Carell ES, Schroth G, Ali A. Circumferential balloon rupture and catheter fracture due to entrapment in a calcified coronary stenosis. Cathet
- Kussmaul WG, Marzo K, Tomaszewski J, DiSesa VJ. Rupture and entrapment of a balloon catheter in the left anterior descending artery: fluoroscopic appearance of impending balloon failure. Cathet Cardiovasc Diagn. 1993; 28(3): 256-259.
- Chang TT, Pellegrini D, Ostrovsky A, Marrangoni A. Surgical management of entrapped percutaneous transluminal coronary angioplasty hardware. Tex Heart Inst J. 2002; 29(4): 329-332.
- Madronero JM, Hein F, Bergbauer M. Managing complications of stenting: removal of a ruptured, detached, and entrapped angioplasty balloon after coronary stenting. J Invasive Cardiol. 2000; 12(2): 102-104.
- Tastan A, Seyithanoglu BY, Ergene O, Belgi A, Kaya D, Kozan O. Entrapment and removal of a broken angioplasty balloon from a chronically occluded coronary artery. J Invasive Cardiol. 1998; 10(1): 45-47.
- Colombo A, Skinner JM. Balloon entrapment in a coronary artery: potential serious complications of balloon rupture. Cathet Cardiovasc Diagn. 1990; 19(1): 23-25.
- Rehman A, Khan JA, Sial JA, Baloch ZH. Device entrapment: a rare complication of percutaneous coronary intervention. J Coll Physicians Surg Pak. 2011; 21(10): 620-22.
- Al-Moghairi AM, Al-Amri AS. Management of retained intervention guide-wire: a literature review. Curr Cardiol Rev. 2013; 9(3): 260-266.
- Doring V, Hamm C. Delayed surgical removal of a guide-wire fragment following coronary angioplasty. Thorac Cardiovasc Surg. 1990; 38(1): 36-37.
- Girish MP, Gupta MD, Mittal A. Percutaneous retrieval of entrapped partially inflated broken coronary angioplasty balloon by modified fogarty technique. J Invasive Cardiol. 2011; 23(7): E173-E176.
