


ADVERTISEMENT
Complex Bifurcation Stenting in the Transradial Era
The following case is the second in a series of transradial-focused reports, directed by section editor Dr. Samir Pancholy. This case series is supported by an educational grant from Medtronic.
Disclosures: Dr. Sawlani reports no conflicts of interest regarding the content herein. Dr. Shroff serves as a consultant to Terumo, St. Jude Medical and The Medicines Company. The authors can be contacted via Dr. Neal Sawlani at nsawlani@uic.edu.
History
A 46-year-old man with a history of three-vessel coronary artery disease presented with increasing angina. He has a history of hypertension, dyslipidemia, and a non-ST-elevation myocardial infarction (NSTEMI) two years ago, at which time he declined coronary artery bypass surgery. He subsequently underwent staged percutaneous coronary interventions of the right coronary (RCA) and left anterior descending (LAD) coronary arteries, and now presents two years later with increasing chest pressure. After his initial percutaneous revascularizations, he was walking 2.5 miles without symptoms, but now he consistently has sub-sternal chest pain with activity. His medications include aspirin 81 mg and prasugrel 10 mg once daily.
Procedure
A single front-wall puncture into the right radial artery was made and a 5 French hydrophilic introducer sheath was advanced over a spring straight 0.021-inch wire (Terumo). Verapamil (1000 mcg) and unfractionated heparin (5,000 U) were administered through the introducer sheath. A 0.035-inch stainless steel “J” tip wire (St. Jude Medical) was advanced to the aortic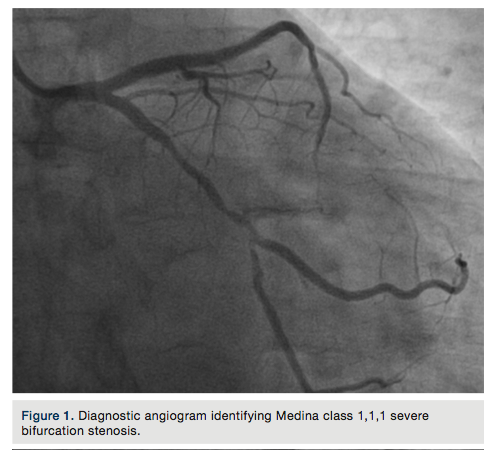 valve cusps and 5 French TIG 4.0 diagnostic catheter (Terumo) was used to engage the right and left coronary arteries. Standard right anterior oblique (RAO) and left anterior oblique (LAO) views demonstrated widely patent stents in the RCA and LAD. The RAO-caudal view identified Medina class 1,1,1 severe bifurcation stenosis in the distal left circumflex and obtuse marginal coronary arteries (Figure 1).
valve cusps and 5 French TIG 4.0 diagnostic catheter (Terumo) was used to engage the right and left coronary arteries. Standard right anterior oblique (RAO) and left anterior oblique (LAO) views demonstrated widely patent stents in the RCA and LAD. The RAO-caudal view identified Medina class 1,1,1 severe bifurcation stenosis in the distal left circumflex and obtuse marginal coronary arteries (Figure 1).
The 5 French diagnostic catheter and sheath were exchanged over the wire for a 6 French hydrophilic introducer sheath (Terumo). A 6 French XBLAD 3.5 guide catheter (Cordis) was advanced over the wire and easily engaged the left main coronary artery. Bivalirudin bolus and infusion were administered with an activated clotting time of 356 seconds. An Asahi Prowater Flex 0.014-inch guide wire (Abbott) was advanced into the main branch beyond the stenosis. Then a Hi-Torque Whisper 0.014-inch guide wire (Abbott) was advanced into the side branch beyond the stenosis.
A Maverick 2 RX 2.5 x 12 mm balloon (Boston Scientific) would not advance beyond the side branch bifurcation lesion. The side branch lesion was predilated with a Sprinter Legend RX 1.25 x 6 mm balloon (Medtronic) followed by a Maverick 2 RX 1.5 x 15 mm balloon and inflated up to 12 atmospheres. The side and main branches were then both predilated with Maverick 2 RX 2.5 x 12 mm kissing balloons (Boston Scientific) up to 10 atm. A Xience Xpedition RX 2.75 x 38mm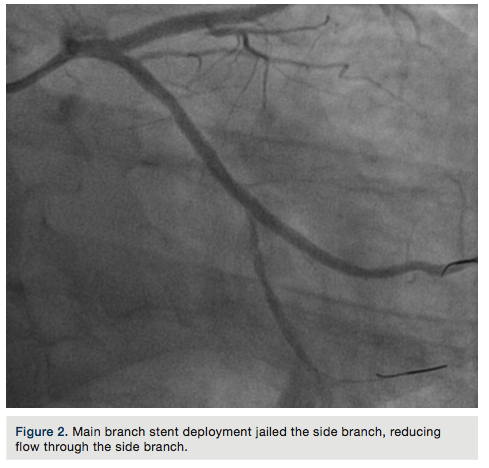 stent (Abbott) was deployed at 14 atmospheres in the main branch, jailing the side branch (Figure 2).
stent (Abbott) was deployed at 14 atmospheres in the main branch, jailing the side branch (Figure 2).
Provisional T-stenting and small protrusion (TAP) bifurcation stenting was performed by rewiring the side branch through the stent struts with a Pilot 50 guide wire (Abbott) and removing the trapped Hi-torque Whisper guide wire. Kissing balloon inflation was performed with two Maverick 2 RX 2.5 x 15 mm balloons (Boston Scientific) — one in the main branch and one into the side branch through the stent struts inflated up to 8 atm. Next, a Xience Xpedition RX 2.5 x 18 mm stent (Abbott) was deployed into the side branch while an uninflated balloon remained in main branch (Figure 3).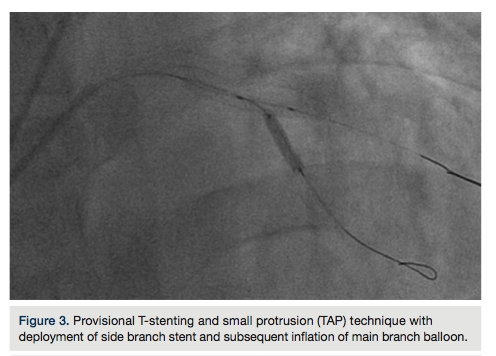
Unfortunately, side branch stenting was complicated by dissection with no distal flow (Figure 4).
To rescue the side branch, an overlapping Xience Xpedition 2.25 x 18 mm stent (Abbott) was deployed distal to the side branch stent at 14 atmospheres. However, intracoronary optical coherence tomography (St. Jude Medical) of the side branch identified a long proximal dissection plane as well (Figure 5).
A Xience Xpedition RX 2.5 x 8 mm stent (Abbott) was deployed at the ostium of the side branch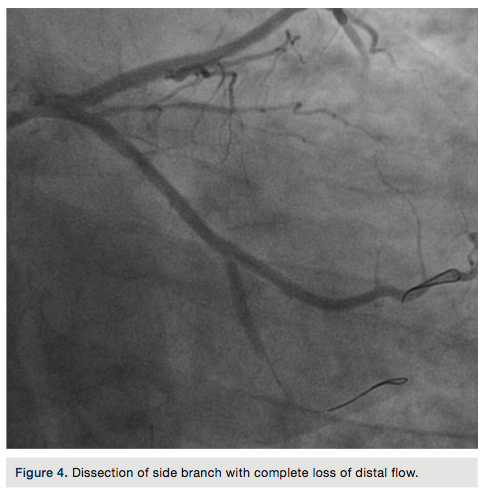 at 14 atmospheres. Simultaneous kissing balloon inflation was performed using the stent balloon and a Maverick 2 RX 2.5 x 15 mm balloon (Boston Scientific) in the main branch at 14 atmospheres.
at 14 atmospheres. Simultaneous kissing balloon inflation was performed using the stent balloon and a Maverick 2 RX 2.5 x 15 mm balloon (Boston Scientific) in the main branch at 14 atmospheres.
Lastly, attention was then turned to post-dilation of the proximal portion of the original main branch stent with an NC Quantum Apex 3.0 x 20 mm balloon (Boston Scientific) at 16 atmospheres. Final angiographic views demonstrated TIMI-3 flow without a dissection flap (Figure 6).
Discussion
Complex coronary bifurcation stenosis is a persistent challenge for experienced operators, with a variety of two-stent techniques available. Randomized trials of bifurcation stenting have suggested that a provisional T-stent approach is preferable to a systemic two-stent strategy.1 Fortunately, 6 French guide catheters are suitable for this strategy and the transradial approach remains a viable option.
This case represents true coronary bifurcation stenting with provisional TAP technique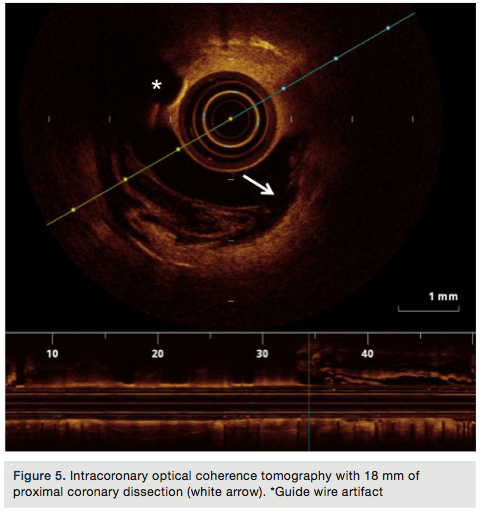 complicated by side branch dissection and ultimately rescued with repeat T-stenting. A two-stent technique was possible through a 6 French transradial strategy without the need for crossover to the femoral approach for larger guide catheter support. Plaque modification was initially achieved by pre-dilating the lesions in order to accommodate stent delivery, including simultaneous kissing balloon inflations. Guide wire selection was instrumental in crossing the stenosis and guide catheter support for stent delivery was certainly adequate.
complicated by side branch dissection and ultimately rescued with repeat T-stenting. A two-stent technique was possible through a 6 French transradial strategy without the need for crossover to the femoral approach for larger guide catheter support. Plaque modification was initially achieved by pre-dilating the lesions in order to accommodate stent delivery, including simultaneous kissing balloon inflations. Guide wire selection was instrumental in crossing the stenosis and guide catheter support for stent delivery was certainly adequate.
Procedural failure is often cited as a limitation to the transradial approach, and is weighed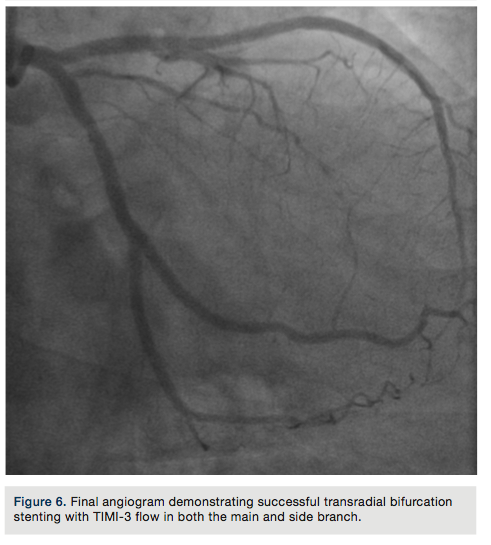 against the advantage of lower access site complications.2 Procedural failure is most commonly cited as being secondary to inadequate guide backup support and difficulty with traversing tortuous anatomy.3 With modern techniques and equipment selection, transradial operators are able to successfully perform complex percutaneous coronary interventions and utilize the full armamentarium of intracoronary imaging devices without access site crossover.
against the advantage of lower access site complications.2 Procedural failure is most commonly cited as being secondary to inadequate guide backup support and difficulty with traversing tortuous anatomy.3 With modern techniques and equipment selection, transradial operators are able to successfully perform complex percutaneous coronary interventions and utilize the full armamentarium of intracoronary imaging devices without access site crossover.
References
- Hildick-Smith D, de Belder AJ, Cooter N, Curzen NP, Clayton TC, Oldroyd KG, et al. Randomized trial of simple versus complex drug-eluting stenting for bifurcation lesions: the British Bifurcation Coronary Study: old, new, and evolving strategies.Circulation. 2010; 121 (10): 1235-1243.
- Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S, Turri M, Anselmi M, et al. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures: systematic overview and meta-analysis of randomized trials. J Am Coll Cardiol. 2004; 44(2): 349-356.
- Dehghani P, Mohammad A, Bajaj R, Hong T, Suen CM, Sharieff W,et al. Mechanism and predictors of failed transradial approach for percutaneous coronary interventions. JACC Cardiovasc Interv. 2009: 2.11: 1057-1064.
